

Introduction
While Multiple myeloma (MM) is a disease of the elderly diagnosed at a median age of 69 years with nearly a third being above the age 75, little is known about the impact of aging processes on either disease biology or clinical outcomes. Treatment decisions are complicated, and it is important to take account three interacting variables: tumor genetics, comorbidities and the efficacy and toxicity of the treatment selected. While frailty scores help stratify elderly MM patients by functional status, quantitative measures of aging could provide biological markers to enhance clinical staging systems, standardize decision making, and guide treatment choices in the elderly MM population. In this work, we characterized the genetics of older MM patients compared to younger patients, and determined the associations of age with clonal hematopoiesis and telomere length (TL), both of which have been shown to be impacted by aging.
Methods
Using the MMRF CoMMpass IA15 data, we analyzed 972 NDMM patients with whole genome long insert sequencing with matching whole exomes. Using paired samples, we determined mutations (Mutect2 and Strelka), copy number (Control-FREEC v. 11.4), translocations (Manta v. 1.4.0), complex rearrangements (ChainFinder and ShatterSeek), as previously described and TL using Telomerecat. Looking at the germline data, we quantified Clonal Hematopoiesis of Indeterminate Potential (CHIP) and quantified TL using the same approach.
Results
The overall survival of patients aged over sixty-five is significantly worse than patients younger than this age (HR 1.7 (CI 95% 1.3-2.3), p<0.0001).
Using a Bayesian approach, we show that, that del(16p) and del(6q) were more frequent in older patients (Corr=0.10, BF=1.1 and Corr=0.13, BF=11). Similarly, mutational signatures did not substantially differ between age groups with the exception of the proportion of APOBEC (SBS2 and 5) which was higher in the group over age > 80 (χ2=11, p=0.02).
We determined both simple and complex structural variants and found that the prevalence of chromothripsis increased with age (χ2=10.8, p=0.001). To determine whether this may be related to chromosomal instability occurring as a consequence of aging we examined the extent of telomere attrition. A significant negative correlation was identified between TL and age (F=9.5, p=0.002) but there were no correlations with complex rearrangements. We did, however, find that TL was significantly shorter in the TP53 (χ2=9, p=0.002) and ATM (χ2=7.2, p=0.007) mutated groups suggesting TL shortening may be associated with DNA instability.
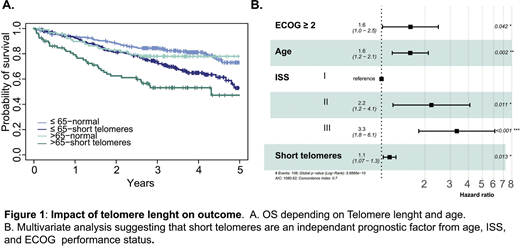
To further determine the association of short TL in malignant plasmacells with adverse outcomes we ranked patients based on TL quartile and determined the impact on outcome for the shortest TL. We show that 14%, 29%, 24%, 29%, and 21% of the >50, 50-60, 60-70-70-80, and >80 year old patients were within this short TL group. There was a significant correlation with adverse overall-survival both in the younger and older patients, Figure 1A.
To understand and quantify the impact of aging of the normal hematopoietic system on outcomes in MM we quantified CHIP and TL on the germline samples. CHIP was seen in 156 patients (16%) and DNMT3A, ASXL1, and TET2 were the more frequent mutations. Patients with CHIP were significantly older (χ2=3.9, p=0.005), as it was seen in 22% of the over 80. The only signatures identified using a fitting approach for these CHIP mutations were the two age related mutational signatures (SBS1 and SBS5). Interestingly, patients with CHIP did not have significantly adverse clinical outcome.
To understand the impact of genetics and markers of aging in the older population we performed a multivariate analysis on the subset of patients over age 65 (n=375). Like others, we found that the well described prognostic genetic risk factors (del(17p), TP53 mutations, t(4;14), t(14;16), and amp1q) did not appear to contribute to the independent assessment of risk when taking into account age, ISS, and performance status (ECOG≥2). We show that in this population of older myeloma that short TL was, however, an independent marker for negative outcome, Figure 1B.
Conclusion:
We highlight the importance of TL, a composite factor that takes into account both DNA instability, copy number losses, and aging as a potential novel biological marker to assess outcome and aid personalized treatment decisions in older patients with MM.
Bauer:Synthekine: Current Employment. Braunstein:Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; TG Therapeutics: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Verastem: Membership on an entity's Board of Directors or advisory committees; Epizyme: Membership on an entity's Board of Directors or advisory committees; Morphosys: Membership on an entity's Board of Directors or advisory committees. Landgren:Amgen: Consultancy, Honoraria, Research Funding; Takeda: Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Janssen: Consultancy, Honoraria, Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Janssen: Consultancy, Honoraria, Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Seattle Genetics: Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Glenmark: Consultancy, Honoraria, Research Funding; Takeda: Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Binding Site: Consultancy, Honoraria; Cellectis: Consultancy, Honoraria; BMS: Consultancy, Honoraria; Karyopharma: Research Funding; BMS: Consultancy, Honoraria; Binding Site: Consultancy, Honoraria; Karyopharma: Research Funding; Merck: Other; Glenmark: Consultancy, Honoraria, Research Funding; Adaptive: Consultancy, Honoraria; Seattle Genetics: Research Funding; Pfizer: Consultancy, Honoraria; Juno: Consultancy, Honoraria; Juno: Consultancy, Honoraria; Cellectis: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Merck: Other. Davies:Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Oncopeptides: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Adaptive Biotech: Honoraria; Sanofi: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene/BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Morgan:Karyopharm: Consultancy, Honoraria; GSK: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Roche: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Honoraria; Janssen: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal